.lesson-duration-container {
background-color: #f0f4f8; /* Szarawe tło dopasowane do reszty strony */
padding: 8px 15px; /* Wewnętrzny odstęp */
border-radius: 8px; /* Zaokrąglone rogi */
font-family: ‘Roboto’, Arial, sans-serif; /* Czcionka Roboto, jeśli dostępna */
font-size: 16px; /* Rozmiar tekstu */
color: #6c757d; /* Ciemny szary kolor tekstu */
display: inline-block; /* Wyświetlanie jako element blokowy */
margin-bottom: 20px; /* Odstęp na dole */
border: none; /* Bez obramowania */
}
.lesson-duration-label {
font-weight: 700; /* Pogrubienie dla etykiety */
color: #6c757d; /* Ciemny szary kolor dla etykiety */
margin-right: 5px; /* Odstęp od wartości */
}
.lesson-duration-value {
color: #6c757d; /* Ciemny szary kolor dla wartości */
font-weight: 700; /* Pogrubienie dla wartości */
}
Functions of the Male Reproductive System
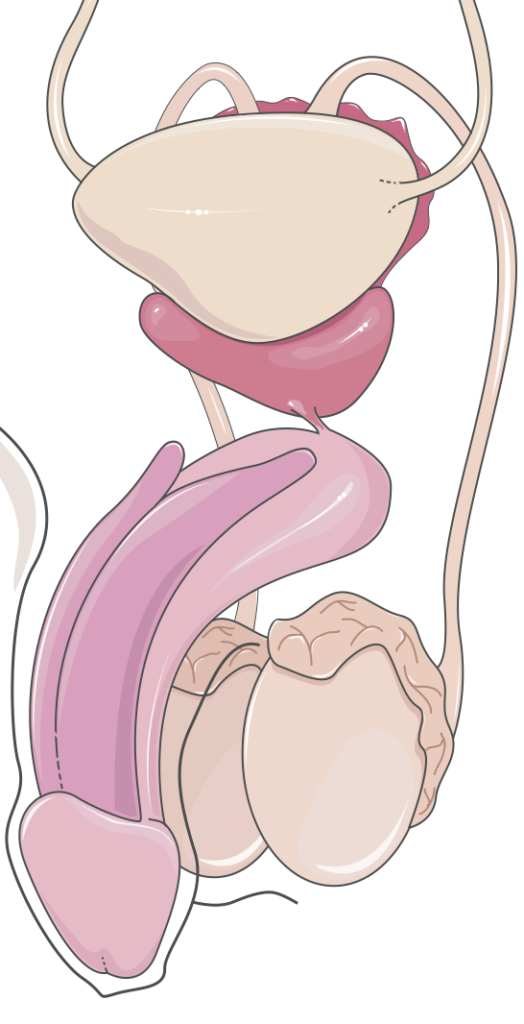
The male reproductive system is responsible for gametogenesis, steroidogenesis, and the delivery of spermatozoa to the female reproductive tract. It is essential for reproduction and maintaining secondary sexual characteristics regulated by testosterone. The primary components of this system include the testes, epididymis, vas deferens, seminal vesicles, prostate gland, and penis, each contributing crucial functions to male fertility and reproductive health. Endocrine, vascular, and structural components coordinate to maintain reproductive function and male health.
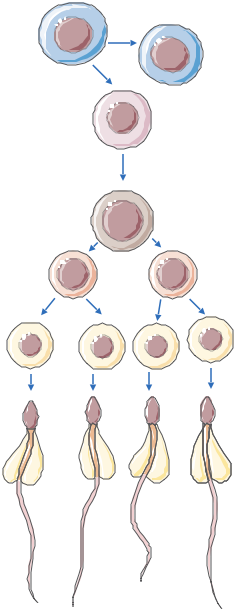
Spermatogenesis
Spermatogenesis occurs in the seminiferous tubules of the testes, producing haploid spermatozoa from diploid germ cells through mitotic and meiotic divisions. This process ensures a consistent supply of genetically diverse gametes capable of fertilization.
Production and Maturation of Sperm
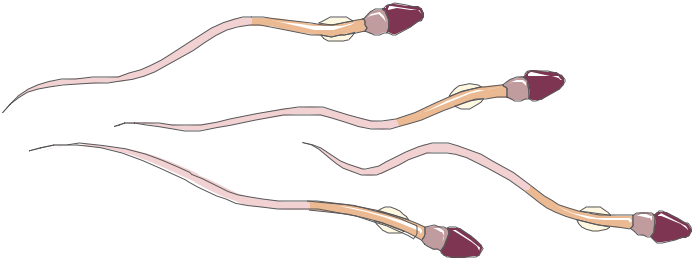
Testicular Function: Spermatogenesis occurs within the seminiferous tubules, beginning with spermatogonia, the diploid germ cells that undergo mitotic proliferation. Spermatogonia differentiate into primary spermatocytes, which initiate meiosis I, producing secondary spermatocytes. These cells proceed through meiosis II to yield haploid spermatids. Spermatids subsequently undergo spermiogenesis, a complex remodeling phase during which they acquire the characteristic morphology of mature spermatozoa, including the development of the acrosome and flagellum. Each stage is crucial for producing viable gametes for fertilization.
Hormonal Regulation: The hypothalamic-pituitary-gonadal (HPG) axis regulates spermatogenesis. Gonadotropin-releasing hormone (GnRH), secreted by the hypothalamus, stimulates the anterior pituitary to release luteinizing hormone (LH) and follicle-stimulating hormone (FSH). LH acts upon Leydig cells to stimulate testosterone production, which is essential for spermatogenesis. FSH acts on Sertoli cells, which provide critical structural and metabolic support to developing germ cells. Sertoli cells produce androgen-binding protein (ABP), which maintains high testosterone levels in the seminiferous tubules. Sertoli cells secrete inhibin to modulate FSH secretion via negative feedback, ensuring precise hormonal control.
Maturation in the Epididymis: Following their release from the seminiferous epithelium, immature spermatozoa are conveyed to the epididymis, where they undergo an extended maturation process over approximately two weeks. Within the epididymis, sperm acquire progressive motility and fertilizing capability, which are crucial for successful oocyte penetration. The epididymal environment modifies the sperm membrane, enhancing stability and functionality. The maturation of sperm in the epididymis is highly dependent on androgenic stimulation, particularly testosterone.
Testosterone Production
Testosterone is the predominant androgen synthesized by the male reproductive system, fundamental for the development of male reproductive structures, maintenance of spermatogenesis, and regulation of secondary sexual traits. Testosterone synthesis is regulated to support reproductive functions and systemic health.
Hormonal Functions
Leydig Cells and Testosterone Synthesis: Leydig cells, located in the interstitial tissue of the testes, are the primary site for testosterone production. LH binding to receptors on Leydig cells activates the cAMP pathway, leading to the enzymatic conversion of cholesterol to testosterone. Testosterone exerts both autocrine and paracrine effects, acting locally to support spermatogenesis and systemically to influence secondary sexual characteristics and anabolic processes, such as muscle hypertrophy and erythropoiesis. Leydig cell function can be affected by factors such as nutrition, stress, and endocrine disruptors.
Role in Sexual Characteristics: During fetal development, testosterone facilitates the differentiation of the Wolffian ducts into the epididymis, vas deferens, and seminal vesicles, defining male reproductive anatomy. At puberty, testosterone drives the development of secondary sexual characteristics, including increased muscle mass, deepening of the voice, and growth of facial, axillary, and pubic hair. Testosterone acts through androgen receptors in target tissues, modulating gene transcription. Testosterone’s influence on somatic tissues extends beyond reproductive functions, encompassing metabolic regulation, skeletal integrity, and overall male phenotype.
Regulation of Libido: Testosterone has a profound impact on male libido and sexual motivation, modulating neuronal activity in brain regions involved in sexual arousal and behavior. Adequate testosterone levels are requisite for normal libido, erectile function, and the maintenance of reproductive health. Testosterone deficiency can lead to reduced sexual desire and erectile dysfunction. Additionally, testosterone exerts neuromodulatory effects on mood, cognition, and general well-being, with hypogonadism often associated with depressive symptoms and reduced quality of life.
Transport and Delivery of Sperm
The transport and delivery of spermatozoa involve a series of well-coordinated anatomical structures and accessory glands, which function collectively to facilitate the movement of sperm from the testes to the female reproductive tract. These ducts and glands ensure that viable sperm reach the site of fertilization.
Pathway of Sperm Transport
Vas Deferens: Mature sperm are stored in the cauda epididymis until ejaculation. During ejaculation, smooth muscle contractions, mediated by sympathetic stimulation, propel sperm through the vas deferens, a muscular tube that serves as the primary conduit from the epididymis to the ejaculatory ducts. The vas deferens’ smooth muscle contracts to ensure efficient sperm transport during ejaculation.
Seminal Vesicles and Prostate Gland: As sperm move through the vas deferens, they are mixed with secretions from the seminal vesicles and prostate gland, which together contribute to the bulk of the ejaculate. The seminal vesicles secrete an alkaline, fructose-rich fluid that serves as an energy substrate for spermatozoa. This fluid also contains prostaglandins, which promote contractions within the female reproductive tract, enhancing sperm motility. The prostate gland produces an alkaline fluid that contains enzymes, including PSA, which helps liquefy semen after ejaculation. Prostatic fluid buffers the acidic female reproductive tract, optimizing sperm viability.
Ejaculatory Ducts and Urethra: The ejaculatory ducts form from the convergence of the vas deferens and seminal vesicle ducts. These ducts merge with the prostatic urethra, and during ejaculation, semen passes through the urethra to be expelled from the penis. The internal and external urethral sphincters play a key role in regulating the passage of semen, ensuring unidirectional flow and preventing retrograde ejaculation into the bladder.
Semen Production
Semen consists of spermatozoa in secretions from accessory glands, supporting sperm viability and motility for fertilization.
Composition and Function of Semen
Seminal Vesicles: The seminal vesicles contribute approximately 60-70% of the seminal fluid volume. Their secretions contain fructose, which provides an energy source for sperm, and prostaglandins, which stimulate smooth muscle contractions in both the male and female reproductive tracts. Seminal vesicular fluid contains proteins that coagulate the ejaculate, aiding semen retention in the female tract.
Prostate Gland: The prostate gland contributes about 20-30% of the ejaculate volume, secreting an alkaline fluid that serves to neutralize vaginal acidity. Prostatic fluid also contains zinc, citrate, and enzymes such as PSA, which help liquefy the coagulum formed by seminal vesicular proteins, allowing sperm to swim freely. Zinc stabilizes chromatin within spermatozoa, ensuring genetic integrity.
Bulbourethral Glands: The bulbourethral glands (Cowper’s glands) produce a clear, mucus-like secretion that is released during sexual arousal. Pre-ejaculate fluid neutralizes residual urethral acidity, providing a favorable environment for sperm. It also acts as a lubricant, facilitating the passage of semen through the urethra.
Erectile Function and Ejaculation
Erectile function and ejaculation involve neurovascular, endocrine, and muscular components. These processes are integral to sexual intercourse and the successful deposition of semen within the female reproductive tract.
Mechanisms of Erection and Ejaculation
Vascular Changes: Penile erection is primarily mediated by increased arterial inflow into the erectile tissues—specifically, the corpora cavernosa. Upon sexual arousal, nitric oxide (NO) is released from parasympathetic nerve endings, leading to the activation of guanylate cyclase in the smooth muscle cells of the penile vasculature. This results in elevated levels of cyclic GMP (cGMP), which decreases intracellular calcium concentrations and causes relaxation of smooth muscle, allowing the corpora cavernosa to fill with blood. Increased intracavernosal pressure leads to penile rigidity, enabling copulation.
Nervous System Regulation: The autonomic nervous system is essential for regulating both erectile and ejaculatory functions. Parasympathetic activation, originating from the sacral spinal cord, is responsible for initiating erection, while sympathetic stimulation, originating from thoracolumbar spinal segments, governs ejaculation. During ejaculation, sympathetic outflow induces rhythmic contractions of the vas deferens, seminal vesicles, and prostate gland, facilitating the movement of semen into the urethra.
Phases of Ejaculation: Ejaculation is a two-phase process comprising emission and expulsion.
During emission, sperm and seminal fluids are transported to the posterior urethra by the coordinated contractions of the vas deferens, seminal vesicles, and prostate.
Expulsion is mediated by the contraction of the bulbospongiosus and ischiocavernosus muscles, resulting in the forceful ejection of semen from the urethral meatus. Coordinated timing ensures effective sperm delivery into the female reproductive tract.
Maintaining the Health of the Male Reproductive System
Maintaining male reproductive health is crucial for fertility and hormonal balance. Managing diet, exercise, and preventive healthcare enhances reproductive outcomes.
Nutritional and Lifestyle Factors
Balanced Diet: A diet rich in essential micronutrients—particularly antioxidants, zinc, selenium, and vitamins E and C—is vital for supporting spermatogenesis and testosterone production. Antioxidants protect sperm from oxidative stress, preventing DNA damage. Foods such as leafy greens, nuts, and seafood provide these critical nutrients, which also support the overall health of reproductive tissues and improve sperm quality.
Physical Activity: Regular physical exercise contributes positively to cardiovascular health, hormonal balance, and erectile function. Endothelial health promotes blood flow to reproductive organs, enhancing testosterone synthesis and erectile function. However, excessive physical activity or the misuse of anabolic steroids can adversely affect the hypothalamic-pituitary-gonadal axis, resulting in suppressed testosterone production and reduced fertility.
Avoidance of Toxins: Exposure to environmental toxins, including pesticides, heavy metals, and endocrine-disrupting chemicals, has been linked to impaired spermatogenesis and decreased testosterone production. Exposure can reduce sperm count, motility, and cause abnormal morphology. Limiting exposure to these substances, along with avoiding excessive alcohol, smoking, and recreational drug use, is critical for maintaining reproductive health.
Preventive Healthcare
Regular Health Screenings: Routine health assessments, including testicular self-exams and STI screenings, are essential for early detection of issues like testicular cancer or varicoceles. Early intervention can significantly improve reproductive outcomes and help prevent long-term complications that may contribute to infertility.
Stress Management: Chronic stress elevates cortisol, suppressing the HPG axis and reducing testosterone production. Stress management strategies—such as mindfulness, meditation, yoga, and physical exercise—are crucial for maintaining optimal reproductive health. Chronic stress impacts hormone levels and contributes to erectile dysfunction and reduced sperm quality.
Zaloguj się
To szkolenie wymaga wykupienia dostępu. Zaloguj się.