Lekcja 7: Kliniczne aspekty chorób skóry 2 | Clinical Aspects of Skin Diseases 2
Psoriasis
Psoriasis is a chronic autoimmune skin condition characterized by the rapid turnover of skin cells, leading to the formation of red, scaly patches on the skin. It primarily affects the scalp, elbows, knees, and lower back but can appear anywhere on the body. The condition is not contagious and is often triggered by factors such as stress, infections, or skin injuries.

Pathophysiology
Psoriasis is a chronic autoimmune condition characterized by rapid turnover of epidermal keratinocytes. The pathogenesis involves:
- Immune dysregulation: Psoriasis is driven by T-cell–mediated inflammation, with Th17 and Th1 cells playing a critical role. These cells release cytokines such as IL-17 and TNF-alpha, which promote the proliferation of keratinocytes and inflammation.
- Genetic predisposition: A family history of psoriasis increases the likelihood of developing the condition, with several genetic loci (e.g., PSORS1) implicated.
- Environmental triggers: Stress, infections, medications (e.g., beta-blockers, lithium), and trauma to the skin (Koebner phenomenon) can precipitate flares.
Clinical Presentation
Psoriasis is marked by well-demarcated erythematous plaques with silvery scales, commonly found on the scalp, elbows, knees, and lower back.
Types of Psoriasis
| Type of Psoriasis | Description |
|---|---|
| Plaque Psoriasis | Thick, red plaques covered with silvery-white scales. |
| Guttate Psoriasis | Small, drop-like lesions, often triggered by streptococcal infections. |
| Inverse Psoriasis | Occurs in skin folds, with smooth, red patches. |
| Pustular Psoriasis | Characterized by white pustules surrounded by red skin. |
| Erythrodermic Psoriasis | A severe, potentially life-threatening form that involves widespread redness and scaling. |
Diagnosis
Diagnosis is clinical, based on the characteristic appearance of plaques. A biopsy may be performed to rule out other conditions in atypical cases. Key histological features include acanthosis (epidermal hyperplasia), parakeratosis(retention of nuclei in the stratum corneum), and Munro microabscesses (collections of neutrophils in the epidermis).
Treatment
Psoriasis treatment is based on the severity of the disease:
- Topical treatments: Corticosteroids, vitamin D analogs (e.g., calcipotriol), and retinoids (e.g., tazarotene) are used for mild to moderate cases.
- Phototherapy: UVB phototherapy or PUVA (psoralen + UVA) is effective for more extensive disease.
- Systemic treatments: For moderate to severe cases, methotrexate, cyclosporine, and biologics targeting TNF-alpha, IL-17, and IL-23 (e.g., adalimumab, secukinumab, ustekinumab) are used.
Complications
Psoriasis is associated with several comorbidities, including psoriatic arthritis, cardiovascular disease, and metabolic syndrome. Psoriatic arthritis affects up to 30% of psoriasis patients and can lead to joint destruction if untreated.
Basal Cell Carcinoma (BCC)
Basal cell carcinoma (BCC) is a common skin cancer originating from the basal cells in the epidermis. It typically manifests as a pearly bump or a flat lesion in sun-exposed areas, such as the face and neck. BCC grows slowly and is unlikely to metastasize, making early detection and treatment important.
OBRAZEK
Pathophysiology
Basal cell carcinoma is the most common type of skin cancer, arising from the basal cells in the epidermis. It is caused by DNA mutations, primarily due to UV radiation exposure, leading to uncontrolled cell growth. BCC is a locally invasive malignancy that rarely metastasizes.
Clinical Presentation
- Nodular BCC: The most common form, appearing as a pearly or translucent nodule with telangiectasia (visible blood vessels) and a rolled border. These lesions are often found on sun-exposed areas such as the face and neck.
- Superficial BCC: Appears as a scaly, red patch and is more commonly found on chest or upper back, arms, or legs.
- Morpheaform (sclerosing) BCC: A more aggressive subtype that appears as a scar-like, ill-defined lesion.
Diagnosis
A clinical diagnosis is typically followed by biopsy to confirm the histopathology. BCC shows basaloid cells in the epidermis, with palisading nuclei and clefts between tumor cells and stroma.
Treatment
- Surgical excision: The treatment of choice for most BCCs, ensuring complete removal with clear margins.
- Mohs micrographic surgery: Often used for high-risk or facial tumors to minimize tissue loss and maximize cure rates.
- Topical therapies: For superficial BCC, imiquimod or 5-fluorouracil may be used.
- Radiation therapy: For patients who cannot undergo surgery.
- Targeted therapy: For advanced or metastatic BCC, vismodegib (a hedgehog pathway inhibitor) is an option.
Prognosis
BCC has an excellent prognosis with appropriate treatment, but recurrence is possible, especially in high-risk or poorly treated cases.
Squamous Cell Carcinoma (SCC)
Squamous cell carcinoma (SCC) is a type of skin cancer that originates in the squamous cells of the epidermis. It commonly appears as a firm, red nodule, a flat sore, or a scaly patch, often on sun-exposed areas such as the face, ears, and hands. SCC can grow more aggressively than basal cell carcinoma and has a higher risk of metastasis if not treated promptly.
OBRAZEK
Pathophysiology
Squamous cell carcinoma arises from keratinocytes in the epidermis and can develop from actinic keratoses, which are premalignant lesions caused by chronic UV exposure. Other risk factors include immunosuppression, HPV infection, and chronic wounds.
Clinical Presentation
SCC typically appears as a firm, red nodule or a scaly, crusted lesion. It may ulcerate or bleed, particularly in sun-exposed areas such as the face, neck, arms, and hands. High-risk SCCs include lesions on the ears, lips, and genitalia, as well as those that are large, deep, or rapidly growing.
Diagnosis
Diagnosis is confirmed by biopsy, revealing atypical keratinocytes extending beyond the epidermis into the dermis. Keratin pearls (whorls of keratinization) are often seen histologically.
Treatment
- Surgical excision with clear margins is the primary treatment.
- Mohs micrographic surgery is preferred for high-risk lesions or those located on the face, hands, or feet.
- Cryotherapy or electrodessication and curettage (ED&C) may be used for superficial SCCs.
- Radiation therapy is an option for patients who are not surgical candidates.
- For advanced or metastatic SCC, systemic chemotherapy or immunotherapy (e.g., cemiplimab, an anti-PD-1 inhibitor) may be used.
Prognosis
SCC has a good prognosis when treated early, but advanced or high-risk cases can metastasize to regional lymph nodes or distant organs.
Melanoma
Melanoma is a type of skin cancer that develops in melanocytes, the cells responsible for producing melanin, the pigment that gives skin its color. While it primarily occurs in the skin, it can also manifest in other parts of the body, such as the eyes, mucous membranes, and rarely in internal organs.
OBRAZEK
Melanoma has seen a steady increase in incidence over the past few decades, especially in regions with high sun exposure. Risk factors include:
- UV Radiation: Overexposure to ultraviolet (UV) radiation, either from the sun or artificial sources like tanning beds.
- Fair Skin: People with fair skin, light-colored eyes, and a tendency to burn rather than tan are at a higher risk.
- Family History: Individuals with a family history of melanoma have an increased risk.
- Multiple Moles: Presence of numerous moles on the body can elevate the risk of developing melanoma.
- Immune Suppression: People with weakened immune systems due to certain medical conditions or medications have an increased susceptibility.
Diagnosis of Melanoma
A dermatologist typically performs a thorough skin examination to evaluate moles for suspicious characteristics. Two widely used systems aid in evaluating suspicious skin lesions: the ABCDE criteria and the Revised 7-Point Checklist. However, a biopsy of the suspicious mole or skin lesion is the definitive method to confirm melanoma.
ABCDE Criteria
This system is commonly employed to identify suspicious moles that may indicate melanoma:
- A – Asymmetry: One half of the lesion differs from the other.
- B – Border: The borders are irregular, notched, or poorly defined.
- C – Color: Variations in color, including different shades of brown, black, or even red, white, or blue.
- D – Diameter: Moles larger than 6 mm (about the size of a pencil eraser) should be examined more closely.
- E – Evolution: Changes in size, shape, color, or symptoms such as itching or bleeding are concerning and should be evaluated promptly.
Revised 7-Point Checklist
This method provides a more structured approach for assessing lesions. It assigns points to major and minor criteria:
- Major Criteria (2 points each): Change in size, shape, or color.
- Minor Criteria (1 point each): Inflammation, crusting or bleeding, sensory changes, and diameter ≥7 mm.
Any patient scoring three or more points on the checklist should be referred for further dermatological evaluation.
Stages of melanoma
Melanoma is divided into stages using five Roman numerals (0 through IV) and up to four letters (A through D) that indicate a higher risk within each stage.
The stages of melanoma are determined mostly by specific details about the tumour and its growth that are tallied in a system called TNM where:
T stands for Tumour,
N stands for Nodes,
M stands for Metastasis.
Staging is important because cancer treatment options and prognoses are determined by stage.
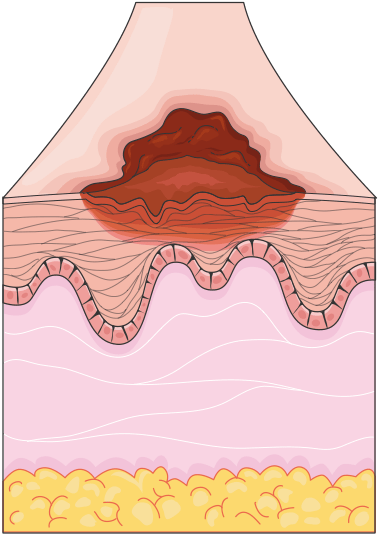
Stage 0 (In Situ): Melanoma is confined to the epidermis, with no invasion of deeper layers.
Figure 1.18, generated using Servier Medical Art, provided by Servier, licensed under a Creative Commons Attribution 4.0 unported license
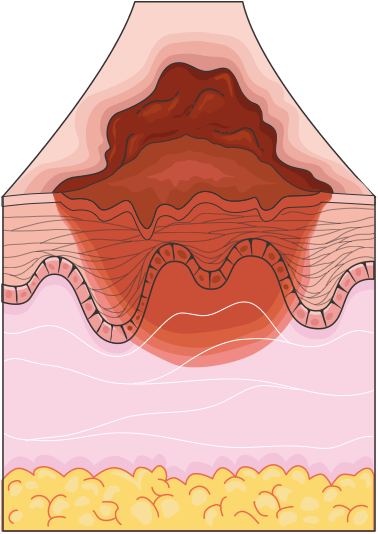
Stage I: Localized melanoma that is still thin, typically measuring 1 mm or less in thickness, confined to the skin.
Stage II: Thicker melanoma (greater than 1 mm) but still localized to the skin, with no lymph node involvement.
Figure 1.19, generated using Servier Medical Art, provided by Servier, licensed under a Creative Commons Attribution 4.0 unported license
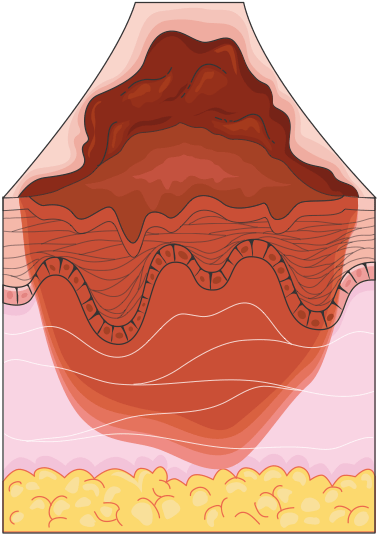
Stage III: Melanoma has spread to nearby lymph nodes or tissues but has not yet reached distant organs.
Stage IV: Advanced melanoma with distant metastases, affecting organs such as the lungs, liver, brain, or bones.
Figure 1.20, generated using Servier Medical Art, provided by Servier, licensed under a Creative Commons Attribution 4.0 unported license
Treatment Options
The treatment of melanoma depends on the stage of the disease:
- Surgical Excision: The primary treatment for localized melanoma involves excising the lesion along with a margin of healthy skin to ensure complete removal.
- Immunotherapy: Drugs like checkpoint inhibitors (e.g., nivolumab, pembrolizumab) are used to enhance the body’s immune response to melanoma cells.
- Targeted Therapy: Used for melanomas with specific genetic mutations (e.g., BRAF mutations), targeted drugs such as vemurafenib or dabrafenib can inhibit cancer cell growth.
- Chemotherapy: While less commonly used for melanoma today, chemotherapy may still be considered in advanced stages or if other treatments are ineffective.
- Radiation Therapy: This may be employed to treat areas of melanoma that have spread, particularly in palliative care settings.
Prevention Strategies
Preventing melanoma revolves around minimizing UV radiation exposure:
- Sunscreen: Regular use of broad-spectrum sunscreen with an SPF of 30 or higher is vital for protection.
- Protective Clothing: Wearing hats, sunglasses, and long sleeves when outdoors provides a physical barrier against UV rays.
- Avoid Tanning Beds: Artificial UV sources increase the risk of melanoma and should be avoided.
- Regular Skin Checks: Patients, especially those with fair skin, a history of sunburns, or a family history of melanoma, should undergo regular skin examinations and self-checks for new or changing moles.