Kliniczne aspekty chorób Układu Powłokowego: część 1 i 2 |Clinical Aspects of Integumentary System diseases: part 1 and 2
Clinical aspects of Skin Health
Skin health can reflect internal health. Changes in skin appearance, texture, and functionality may indicate underlying medical conditions:
- Chronic inflammation: Persistent redness or swelling can indicate autoimmune diseases, infections, or allergies.
- Skin pigmentation shifts: Jaundice (yellowing) may indicate liver issues; pallor (paleness) could signal anemia or circulation problems.
- Texture and hydration imbalances: Dryness or roughness can indicate thyroid issues, diabetes, or nutritional deficiencies.
- Rashes and lesions: Unexplained rashes may signal infections, allergies, or immune disorders like lupus or psoriasis.
- Unusual sensitivity: Skin reactions to products may indicate atopic dermatitis, hormonal changes, or other systemic issues.
Acne Vulgaris
Acne is a multifactorial skin condition affecting the pilosebaceous units (hair follicles and associated sebaceous glands). It primarily manifests during adolescence but can affect individuals at any age. It ranges from mild to severe forms, and if left untreated, can lead to significant scarring and psychological impacts.
Etiology and Pathogenesis
Acne arises from a combination of four main factors:
- Follicular hyperkeratinization: Increased production and retention of keratinocytes within the follicle cause a blockage, leading to comedone formation.
- Increased sebum production: Androgens stimulate sebaceous glands, leading to excess sebum that contributes to follicular blockage.
- Bacterial colonization: Propionibacterium acnes (now called Cutibacterium acnes), a commensal organism, proliferates in the anaerobic environment of the blocked follicle, triggering inflammation.
- Inflammatory response: The immune system responds to Cutibacterium acnes, producing cytokines and enzymes that contribute to inflammation.
Clinical Presentation
Acne lesions are categorized into two main types:
- Non-inflammatory lesions: These include open comedones (blackheads) and closed comedones (whiteheads). Both are caused by the plugging of the follicle with keratin and sebum.
- Inflammatory lesions: Papules, pustules, nodules, and cysts occur when the follicle ruptures, leading to an inflammatory response. Nodules and cysts are deeper, more severe lesions that often lead to scarring if untreated.
Grading of Acne Severity
| Severity | Description |
|---|---|
| Mild Acne | Primarily consists of comedones with occasional papules and pustules. |
| Moderate Acne | Increased numbers of papules and pustules, with possible nodules. |
| Severe Acne | Nodulocystic lesions that can be widespread, painful, and prone to scarring. |
Treatment
- Topical: Retinoids (e.g., tretinoin) to increase cell turnover, benzoyl peroxide for antimicrobial effects, and antibiotics (e.g., clindamycin) to reduce inflammation.
- Oral: Antibiotics (e.g., doxycycline) for moderate to severe cases to decrease bacterial load, isotretinoin for severe nodulocystic acne to reduce sebum production and normalize skin cell turnover, and hormonal treatments (e.g., oral contraceptives, spironolactone) for women to regulate androgen levels.
- Adjunctive: Chemical peels to exfoliate and reduce hyperpigmentation, laser therapy to target scars and reduce inflammation, and steroid injections for deep nodules to reduce swelling and accelerate healing.
Complications
- Scarring: Can occur in severe cases, including both hypertrophic (raised) and atrophic (depressed) scars.
- Post-inflammatory hyperpigmentation (PIH): A common sequela, especially in individuals with darker skin types.
Prognosis
- Mild Acne: Generally has a good prognosis and often resolves with proper topical treatments. Early intervention reduces the risk of scarring and post-inflammatory hyperpigmentation (PIH).
- Moderate to Severe Acne: Requires more aggressive treatment to prevent long-term complications. Isotretinoin has proven highly effective for severe cases but must be monitored due to potential side effects. Psychological impacts, including decreased self-esteem and anxiety, should not be underestimated.
Atopic Dermatitis (Eczema)
Atopic dermatitis (AD) is a chronic, relapsing inflammatory skin disease characterized by intense pruritus (itching) and a defective skin barrier. It commonly affects children but can persist into adulthood. AD is associated with other atopic conditions such as asthma and allergic rhinitis, constituting what is known as the “atopic triad.”
Etiology and Pathogenesis
Atopic dermatitis is thought to result from a combination of genetic, environmental, and immunological factors:
- Genetic predisposition: Mutations in the filaggrin gene (FLG), which plays a crucial role in maintaining skin barrier function, have been associated with atopic dermatitis. This impaired barrier increases skin permeability to allergens and microbes.
- Immune dysregulation: Patients with AD have a heightened Th2 (T-helper cell type 2) immune response, leading to increased production of IgE and subsequent allergic inflammation.
- Environmental factors: Dry climates, exposure to allergens (e.g., dust mites, pet dander), and irritants (e.g., soaps, fragrances) exacerbate the condition.
Clinical Manifestations
- Erythema, edema, and scaling: These are hallmark signs of acute flare-ups.
- Lichenification: Due to chronic scratching and rubbing, the skin becomes thickened.
- Pruritus: Intense itching leads to a scratch-itch cycle and excoriation.
- Location: In infants, AD typically affects the face, scalp, and extensor surfaces. In older children and adults, the flexural areas (e.g., elbows, knees, wrists) are more commonly involved.
Treatment
- Topical: Emollients to restore the skin barrier, topical corticosteroids for inflammation control, and calcineurin inhibitors (e.g., tacrolimus) for sensitive areas to reduce inflammation.
- Oral: Antihistamines for itch relief, oral corticosteroids for severe flares, and biologics (e.g., dupilumab) for moderate to severe refractory cases.
- Lifestyle: Avoiding triggers (e.g., soaps, allergens) and maintaining regular moisturizing routines.
Complications
- Infection: Staphylococcus aureus colonization is common in AD patients, often exacerbating inflammation. Herpes simplex virus can also cause eczema herpeticum, a potentially serious complication.
- Sleep disturbance and psychological stress: Severe itching can lead to insomnia and secondary psychological effects.
Prognosis
- Children: Many children experience improvement as they age, and some may outgrow the condition entirely. However, a significant subset will have intermittent flares throughout their lives.
- Adults: Often face a chronic course with periodic flares. Effective management can greatly improve the quality of life, though complications like sleep disturbances and psychological stress may persist.
Contact Dermatitis
Contact dermatitis is an inflammatory skin condition caused by direct skin exposure to an irritant or allergen. It is divided into two categories: irritant contact dermatitis (ICD) and allergic contact dermatitis (ACD).
Comparison of ICD and ACD
| Characteristic | Irritant Contact Dermatitis (ICD) | Allergic Contact Dermatitis (ACD) |
|---|---|---|
| Etiology | Direct damage to the skin barrier due to exposure to irritants such as detergents, acids, alkalis, solvents, or prolonged water exposure. | Delayed hypersensitivity reaction (Type IV) triggered by exposure to allergens like nickel, fragrances, latex, or plants (e.g., poison ivy). Re-exposure triggers immune response after sensitization. |
| Clinical Presentation | Erythema, dryness, scaling, and fissuring at the site of contact. Symptoms develop within minutes to hours after exposure. Chronic exposure may cause skin thickening and lichenification. | Erythema, vesicles, and intense pruritus at the site of contact. Lesions may spread beyond the initial area of exposure. |
| Onset of Symptoms | Rapid onset (minutes to hours) after exposure to irritants. | Delayed onset (hours to days) following exposure to the allergen. |
| Common Triggers | Detergents, soaps, acids, alkalis, solvents, prolonged water exposure. | Nickel, fragrances, latex, poison ivy, or other sensitizing agents. |
| Chronic Manifestations | Thickening and lichenification of the skin with repeated exposure. | Can recur upon re-exposure to the allergen, may lead to chronic eczematous dermatitis. |
Management
- Identification and Avoidance: Avoidance of the causative irritant or allergen is key. Patch testing may be used to identify specific allergens in allergic contact dermatitis (ACD).
- Topical: Topical corticosteroids to reduce inflammation and itching in both ACD and irritant contact dermatitis (ICD). Emollients are important for restoring the skin barrier, particularly in ICD, where the barrier has been compromised by irritants.
- Oral: Oral corticosteroids are reserved for severe or widespread ACD, particularly when topical treatments fail. Antihistamines may help control itching, though they are more effective in ACD than ICD.
Complications
- Chronic Dermatitis: Repeated exposure to irritants or allergens can lead to chronic dermatitis, characterized by thickened, scaly skin, fissures, and persistent itching.
- Secondary Infections: Damaged skin may become secondarily infected, particularly in cases of severe pruritus leading to excoriation.
Prognosis
- ICD: Often resolves after eliminating the irritant, but chronic exposure can lead to long-term skin thickening and irritation.
- ACD: Symptoms may recur with repeated allergen exposure, but effective avoidance and treatment usually lead to a favorable outcome. Severe or unmanaged cases may result in chronic skin issues, requiring long-term care.
Burn Injuries
Burn injuries, a complex spectrum of skin trauma, demand precise classification and strategic management to optimize patient outcomes. Comprehensive knowledge of burn types, depth assessment, and tailored interventions is crucial in mitigating morbidity and facilitating effective healing.
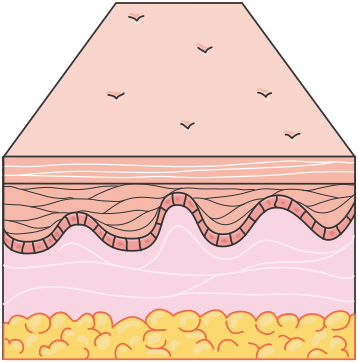
Figure 1.20, generated using Servier Medical Art, provided by Servier, licensed under a Creative Commons Attribution 4.0 unported license
Categorizing Burn Injuries
Burn injuries can be classified based on the cause of the burn. The most common categories include thermal, chemical, electrical, and radiation burns.
| Burn Type | Cause | Details |
|---|---|---|
| Chemical Burns | Exposure to corrosive substances such as acids, alkalis, or industrial compounds | Severity depends on the chemical’s nature, concentration, and duration of skin contact. Alkalis penetrate deeper and cause more damage than acids |
| Electrical Burns | Passage of electrical current through the body | Visible skin damage may be minimal, but internal injuries can be severe, affecting deep tissues, nerves, and organs |
| Radiation Burns | Prolonged exposure to ionizing radiation | Typically slower to develop; damage extends deep into underlying tissues depending on dose and duration of exposure |
Assessing Burn Severity
First-Degree Burns: These are superficial burns affecting only the epidermis. They present with erythema (redness), mild swelling, and pain. First-degree burns typically heal within 3 to 7 days without scarring. An example of a first-degree burn is a mild sunburn.
Figure 1.21, generated using Servier Medical Art, provided by Servier, licensed under a Creative Commons Attribution 4.0 unported license
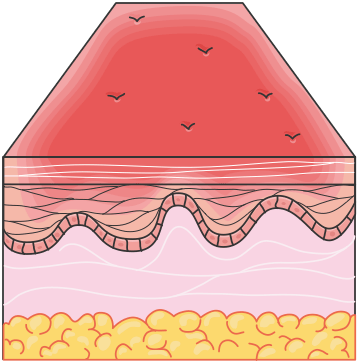
Second-Degree Burns: These burns extend into the dermis and are subdivided into:
- Superficial second-degree burns: Involve the upper layer of the dermis, characterized by blistering, intense pain, and moist, red wounds. Healing usually occurs within 10 to 14 days, with minimal scarring.
- Deep second-degree burns: Penetrate deeper into the dermis, causing more extensive damage. These burns are less painful due to nerve damage and may take 3 to 8 weeks to heal, often leaving scars or requiring skin grafts.
Figure 1.22, generated using Servier Medical Art, provided by Servier, licensed under a Creative Commons Attribution 4.0 unported license
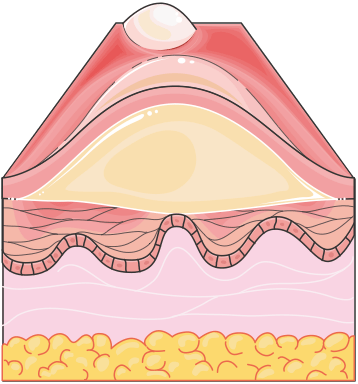
Third-Degree Burns: Also known as full-thickness burns, these injuries involve the complete destruction of the epidermis and dermis, extending into the subcutaneous tissue. The skin may appear charred, leathery, or white. Third-degree burns are typically painless due to nerve destruction, and they require surgical intervention, such as debridement and skin grafting, for proper healing.
Figure 1.23, generated using Servier Medical Art, provided by Servier, licensed under a Creative Commons Attribution 4.0 unported license
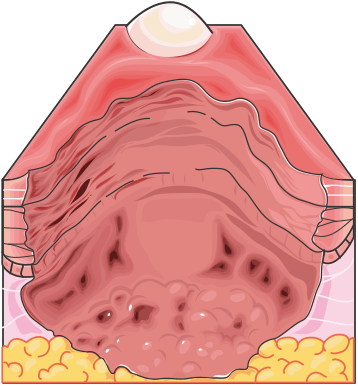
Fourth-Degree Burns: These burns go beyond the skin, damaging underlying muscles, tendons, and bones. They are life-threatening and always require extensive surgical intervention.
Extent of Burn Injuries
- Minor Burns: Limited to smaller areas, usually superficial, akin to mild sunburns.
- Moderate Burns: Extending over larger areas, typically involving second-degree burns or limited third-degree burns.
- Severe Burns: Extensive injuries encompassing substantial body surface area, potentially leading to systemic complications like fluid loss, infection, and shock.
Extent of Burn Injuries: The Rule of Nines
Evaluating the extent of a burn is crucial for determining treatment strategy, especially in severe cases. The Rule of Nines is a quick method for estimating the total body surface area (TBSA) affected by burns. It divides the body into sections, each accounting for a percentage of the total surface area.
- Head and neck: 9%
- Each upper limb: 9% (18% total for both)
- Front trunk: 18%
- Back trunk: 18%
- Each lower limb: 18% (36% total for both)
- Genital area: 1%
Note: Burns affecting 10 percent of a child’s body and those affecting 15 to 20 percent of an adult’s body are considered to be major injuries and require hospitalization and extensive rehabilitation.
Clinical Management of Burn Injuries
1. Immediate Management
- Cooling the Burn: Immediately cooling the affected area with cool (not cold) water for 10 to 20 minutes can help limit the depth of injury. Ice should not be applied, as it can exacerbate tissue damage.
- Removing Constrictive Items: Jewelry, tight clothing, and other constrictive items should be carefully removed to prevent circulation problems due to swelling.
- Sterile Dressings: Burns should be covered with sterile, non-stick dressings to protect the wound from contamination and reduce pain. Specialized burn dressings are often used to maintain a moist wound environment, which promotes healing.
2. Fluid Resuscitation
In cases involving extensive burns (particularly >20% TBSA), rapid fluid loss can lead to hypovolemic shock. Adequate fluid resuscitation, often using the Parkland formula, is essential:
- Parkland formula: 4 mL of lactated Ringer’s solution × body weight (kg) × TBSA (%) = fluid to be administered over the first 24 hours.
- Half of the total fluid is given in the first 8 hours post-injury, with the remaining half administered over the following 16 hours.
3. Wound Debridement and Care
- Debridement: Removal of dead and damaged tissue is essential to prevent infection and facilitate healing. This can be done through surgical, enzymatic, or mechanical methods.
- Topical Antimicrobials: Silver sulfadiazine or mafenide acetate may be applied to burn wounds to prevent infection.
4. Surgical Interventions
- Skin Grafting: For deep second-degree and third-degree burns, skin grafting may be required. Autografts (skin taken from another area of the patient’s body) are preferred, but allografts or synthetic materials may be used in certain cases.
- Escharotomy: In full-thickness burns, the formation of eschar (a hard, dead tissue) can restrict blood flow, particularly in circumferential burns. Escharotomy (surgical removal of eschar) may be necessary to restore circulation and prevent tissue death.
Complications of Burn Injuries
- Infection: The skin serves as the primary barrier against pathogens, and burns compromise this barrier, increasing the risk of infection, including sepsis.
- Hypovolemic Shock: Severe burns can lead to significant fluid loss, resulting in low blood pressure and shock.
- Scarring and Contractures: Deep burns can result in significant scarring, and contractures (permanent tightening of skin) may occur, particularly over joints, leading to restricted movement.
- Systemic Inflammatory Response Syndrome (SIRS): Severe burns can trigger a systemic inflammatory response, leading to organ dysfunction.
Prognosis
- First and Second-Degree Burns: Generally heal well with appropriate care. Superficial burns rarely cause lasting damage, but deeper second-degree burns may leave scars.
- Third and Fourth-Degree Burns: These carry a high risk of complications, such as infections and contractures. Recovery depends on the extent of the burn and can require long-term rehabilitation, including physical and psychological support to address scarring and functional limitations.